
‘Half in love with easeful Death’
Stray thoughts on voluntary euthanasia/assisted suicide

The bleak title above is from a beautiful poem, one which captures the complexity surrounding legislation—now widely called “the Leadbeater Bill”—currently making its way at breakneck speed through the UK’s House of Commons.
Those of you who’ve followed my involvement in public debate over the years would be aware that I’ve supported legalisation of voluntary euthanasia/assisted suicide/etc. You will note the prominence of the Australian parliamentarian for whom I used to be Senior Adviser on this point.
These days, it’s called various different names by both supporters and opponents, and I’m no longer sure which is considered kosher, if any. When I first participated in debates around the issue, “voluntary euthanasia” was the term. For many years, the most prominent campaigning organisation in Australia on this issue was the Northern Territory Voluntary Euthanasia Society.
This emerged because Australia’s Northern Territory—remember the word “territory” in this context, it’s important—attempted to enact voluntary euthanasia legislation in the 1990s, and was promptly overruled by the Federal government. Those of you from federal systems (USA, Germany, Canada etc) are probably raising your eyebrows at this point, given criminal law is generally a matter for the several states.
The Northern Territory, however, was and is a territory, not a state of the Australian Federation. Under Section 122 of the Constitution of Australia the Federal Parliament has the power to override any law passed by a territory parliament. This is what happened in 1997, when the Federal Parliament passed the Euthanasia Laws Act 1997, originally introduced as a private member’s bill by Liberal MP Kevin Andrews.
The irony of Andrews’s intervention is that, as Australia’s states have legalised voluntary euthanasia in various forms, it’s still illegal in the Northern Territory. This kind of thing in federal systems is sometimes described as “the laboratory of the states”. I’m only half-joking. It often works.
It doesn’t take much poking around to reveal that Andrews’s behaviour during this imbroglio was pretty bad, up to and including using rules attaching to private members’ bills to get his way. Because he was a Victorian MP, this contributed to the centre-right finishing up absolutely on the nose in Victoria and was one issue among many that helped Dan Andrews stay in power for as long as he did (and Labor stay in power as long as they are, still).
Given that background, what’s my view of the Leadbeater Bill here in the UK? I don’t have a principled opposition to voluntary euthanasia. I think, like all of these things, it can be done well or badly. However, one thing that’s become very clear since—and sometimes before cough Gender Recognition Act 2004 cough—the Law Lords were removed from Parliament and ensconced in a fancy building called “the Supreme Court” is that a number of astonishingly badly drafted pieces of legislation have made their way onto the statute books.
Is this true of the Leadbeater Bill?
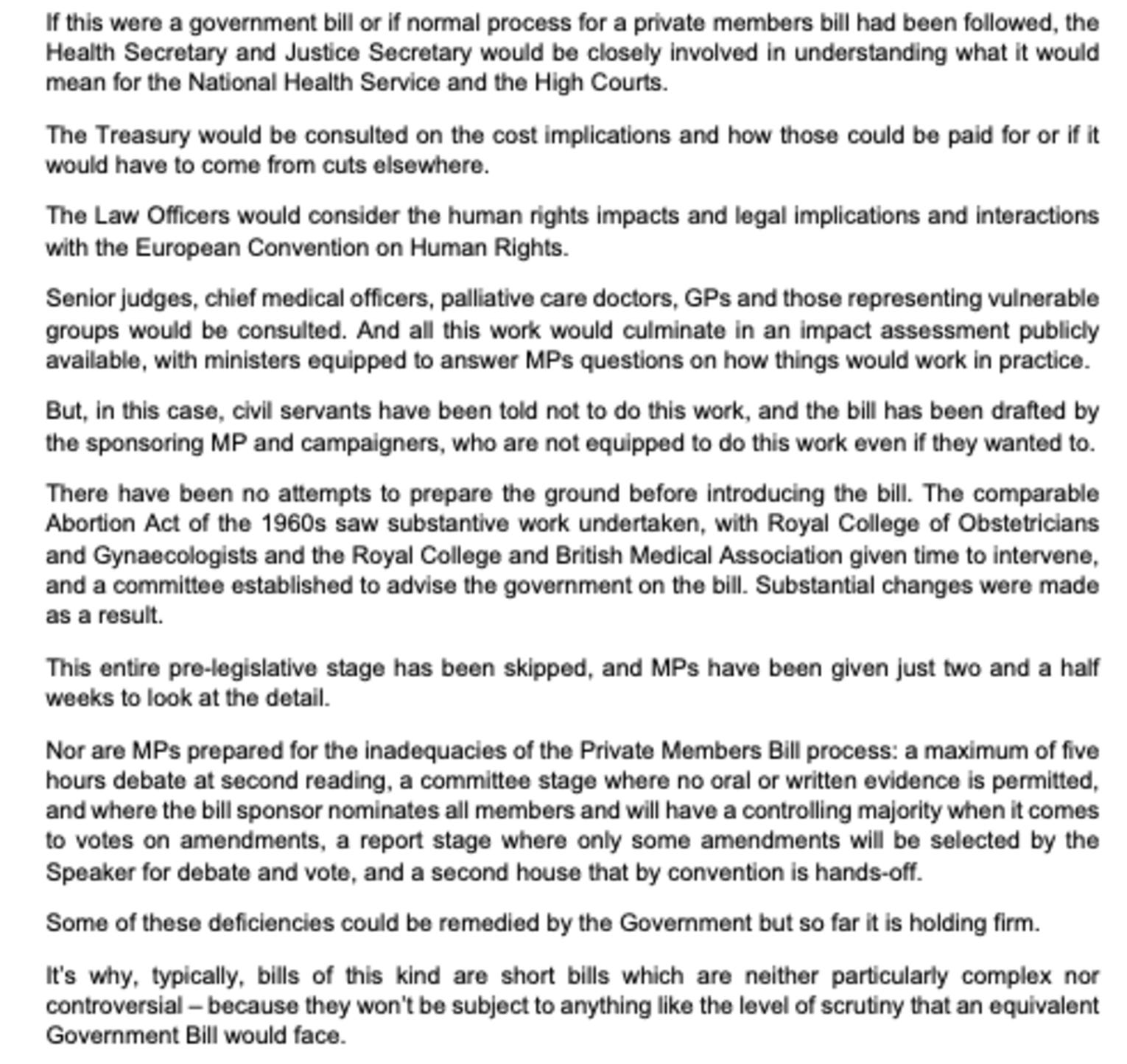
On this point, I’ll defer to someone who’s done a similar job to mine, but in the House of Commons. Nikki da Costa is clearly opposed to voluntary euthanasia in principle as well as to the substance of this particular Bill. However, even though I disagree with her on the principle, I agree that you cannot have this enacted into law without more parliamentary and ministerial scrutiny. I’ve extracted the key passage from Da Costa below, but her whole statement (it’s short) is worth reading:
Had I gone to my old parliamentarian boss in Australia with an agreement from the PM to have my boss’s voluntary euthanasia private members’ bill debated in the Senate—but only for five hours, thereafter to have what Australian senate standing orders calls the guillotine imposed—I strongly suspect he would have withdrawn his support for a crucial piece of government legislation (that being the quid pro quo he offered in order to get parliamentary time) and demanded a proper (longer) debate.
Senator Leyonhjelm supported voluntary euthanasia. He also supports—if anything, even more strongly—clear and transparent debate.
The fact remains that this Bill was drafted entirely by one side—those in favour. That said, it was worked up by Dame Elizabeth Gardiner, who came to it off the back of 10 years as Parliamentary Counsel. For that reason, I’m sure she would have no difficulty with her drafting being exposed to further parliamentary scrutiny, including from the sort of committee da Costa describes with respect to the UK’s 1967 Abortion Act.
Parliamentary matters aside, I would like to make three other observations on this issue.
First, I agree with Ian Leslie that the advertising campaign Dignity in Dying has plastered all over Westminster tube station is, ahem, vomitous:
This is one of a series of posters that adorn the walls of Westminster Underground station, through which many MPs and aides travel to work. On Friday, MPs will be voting on whether or not to legalise assisted dying. The posters, funded by a campaign group called Dignity In Dying, present a series of individuals happily contemplating the prospect of ending their own lives. The vibe is feel-good, joyful and glossy, somewhere between a cosmetics brand and Kamala Harris ‘24. I think they are the creepiest ads I’ve ever seen.
If you wish to encounter a thoughtful but nonetheless morally complex visual and auditory argument for assisted suicide, you would be better off watching Clint Eastwood and Hilary Swank’s 2004 film Million Dollar Baby.
Secondly, the back and forth over “slippery slopes” is not being managed at all well by either side. Slippery slopes are real (sorry, philosophers). On this issue, it’s clear that Canada’s MAID system has whizzed down the slippery slope, and that at least to some degree it’s being used to bump off poor but expensive oldies. Yuan Yi Zhu—a Canadian lawyer now working in the Netherlands—has written widely across various publications about the ongoing problems with Canada’s rapidly loosening criteria for those who seek assisted suicide.
However, attempts to suggest that all voluntary euthanasia regimes around the world are slip-sliding-away-and-down with Canada have been unsuccessful. Critics have suggested problems with Oregon in the US (Kim Leadbeater MP’s favoured comparator) and the Netherlands. To my eye, the evidence is equivocal, with some evidence of “special cases” going awry in Netherlands. There have been relatively few criticisms of Switzerland or Australia.
Why have slopes been slippery in (especially) Canada and the Netherlands? Why are other countries different, with different outcomes? Legislation will vary from country to country, of course, remembering the Netherlands is a Roman-Dutch law jurisdiction, Canada is a common law jurisdiction (as are Australia and Oregon), while Switzerland is wholly civilian. That said, the decision that led to much of Canada’s recent expansion of access to voluntary euthanasia was brought down in a Quebec court. Quebec, like Scotland, has a mixed legal system.
This kind of question is capable of being answered, and answered in such a way that would help legislators, but not in the time allocated to the Leadbeater Bill. This leads me back to Nikki da Costa’s point above. It’s possible that Australia and Switzerland are protected—as is so often the case—by their high state capacity. Which, of course, should enjoin even further caution in the UK. One thing the immigration fustercluck in this country since 2019 has demonstrated—coupled with an inability to build absolutely anything near anyone—is that Blighty is a bit short on the state capacity front.
Thirdly, one of the reasons both sides are arguing past each other in increasingly deranged ways is that both adhere to ethical systems that do not scale. Utilitarianism does not scale down, and virtue ethics doesn’t scale up. This is what’s behind the awful (pro-VE) Westminster tube ads, but also behind the increasingly desperate, covid-lockdown-style claim from anti-VE types: “but that means you want to kill granny”.
Those in favour of voluntary euthanasia tend to draw on consequentialist arguments. That is, they’re applying what is a useful (and very common) heuristic for analysis and assessment when dealing with the implications of a given policy for large numbers of people. It’s difficult to be anything other than utilitarian if your core question is, “but what works here for all these people?” Utilitarianism is famously associated with economics (which tends to be discussed and deployed at scale, natch) and its focus on the importance of trade-offs.
However, take the trade-offs upon which economics and many other wonkish analytical systems depend and apply them in your individual life, you are likely to behave like Sam Bankman-Fried and sound like Matthew Parris:
I don’t dispute the objectors’ belief that once assisted dying becomes normalised we will become more apt to ask ourselves for how much longer we can justify the struggle. Is life still giving us more pleasure than pain? How much is all this costing relatives and the health service? How much of a burden are we placing on those who love us? How much of a burden are we placing upon ourselves? We will notice others asking themselves these questions and we’ll feel empowered by changing social norms to ask them ourselves. Discussion will become more open. It will become common practice to pose this question without embarrassment, and to weigh the answer up.
Virtue ethics, meanwhile—which is guiding team anti-VE—has the opposite problem. It’s a wonderful system when used to help organise your individual moral life. Do virtue ethics properly and you will finish up a better person. Applied at scale, however, it produces things like Prohibition, the Spanish Inquisition, or Twelver Shia Islam in Iran. You may well be able to think, feel, and act well in some domain of your life, or even all domains. But the idea that you can do that on behalf of others, or mandate it for others, in large number—well, I have doubts.
Maybe both these ethical systems are necessarily incomplete. Sometimes virtue ethicists will be right: the law condemns murder outright and doesn’t attempt to “manage” it. It remains always and everywhere illegal. Sometimes consequentialists will be right: prohibition of both drugs and alcohol produces such terrible violence that policing becomes impossible. More people die thanks to that violence and organised crime than would die if drugs and alcohol were legal and regulated. This does not make the latter policy solution ideal or even moral, but it does rule out legislation directed at collective virtue. There is a reason economists hate black markets.
Finally—and yes, I recognise that consequentialist arguments can sound unpersuasive because when applied by/to an individual they do seem mechanical and inhuman—the people (like Matthew Parris) who make them are not Hitler (or Putin). Memes for both allegations are available, note.
The most powerful argument in favour of voluntary euthanasia is that any coercion arising from the legislation in some instances will be outweighed by the end-of-life suffering prevented in most instances elsewhere. This is a classic example of the “economic way of thinking”, and shares roots with concepts like trade-offs and opportunity costs. It’s a claim that can be tested, too, at least comparatively among all those different jurisdictions. If only parliament had time…
More widely, attempting to defeat a claim by pointing out that Hitler made the same or a similar claim is closer to exorcism than argument. I’ve spent years watching people trying to do down vegetarianism because Hitler was one of those, too. Stop it, it’s juvenile.
I hope the Terminally Ill Adults (End of Life) Bill falls in a heap, and Labour then goes away and has a think about how to do this kind of thing properly.
Thanks, Helen. Like you, in principle, I support people being able to make a decision, under certain limited circumstances, to choose to die in the most effective and peaceful way possible, with the assistance of doctors and pharmacists. I have held this view for years. However, I see the legislature and judiciary of the UK as being far closer to Canada, Belgium and the Netherlands than to Australia or Switzerland. From my point of view, I see - as a result of the very poor procedure you outline perfectly - the "slippery slope" being not a bug, but a feature. I also have a slightly modified version of "better that ten guilty people go free than one innocent be punished" pushing to the front of my mind, to the effect of "better ten people who want to die are denied than one who wishes to live feel they should die". I don't think this is either virtue ethics, nor Consequentialism, but I could be wrong. A recent report showing that husbands kill their terminally ill wives at a far higher rate than the other way around leaves me even more nervous about the proposed legislation. This is major legislation, and needs to be approached differently than it is.
Having looked through the bill, it is a dog's dinner tbh. So I am more annoyed by the process than the principle. I have no issues with the Swiss model which is more honest than most around the world. However Leadbeater's private members bill is a dishonest bill of goods and doesn't understand the legal framework it is meant to be operating under.
For example, with the Mental Capacity Act and the Gillick judgment, the NHS assumes that 16 year olds have capacity to consent to medical procedures. The bill reports to be for adults but that won't survive contact with the MCA/Gillick. My expectation is that a 13yo with capacity and a terminal diagnosis could successfully get court approval to end their life.
I am not sure whether it is dishonesty or ignorance but it doesn't fill me with confidence.
I fully agree with you on UK state capacity to deliver this is very weak especially as we have both a social care crisis and a palliative system dependant on charity. That's going to push the UK towards Canadian type statistics where the poorest percentiles are disproportionately represented.
I also don't like the 6 months qualifier threshold. Not only because only one in three deaths will fall within that timeframe but also others can experience unbearable suffering yet be a long way away from their death. The methodology is flawed and itself cruel. If we are to have "assisted dying" then we need a more sophisticated approach that respects people's choices.
If we are to have this in England and Wales then I would suggest that a) the initial period would only see private providers b) NICE (National Institute for Clinical Excellence) run a longitudinal study on those private providers c) a sunset clause on the initial act. Parliament can debate the findings of the longitudinal study and decide whether to extend the policy into the NHS, keep the current arrangement or let the practice end. It would need at least ten years for the study to be meaningful so perhaps a sunset clause of twelve years would be appropriate?
I don't particularly have confidence in Parliament, government, NHS or other parts of the public estate to get this right sadly.